Audiological Presentation
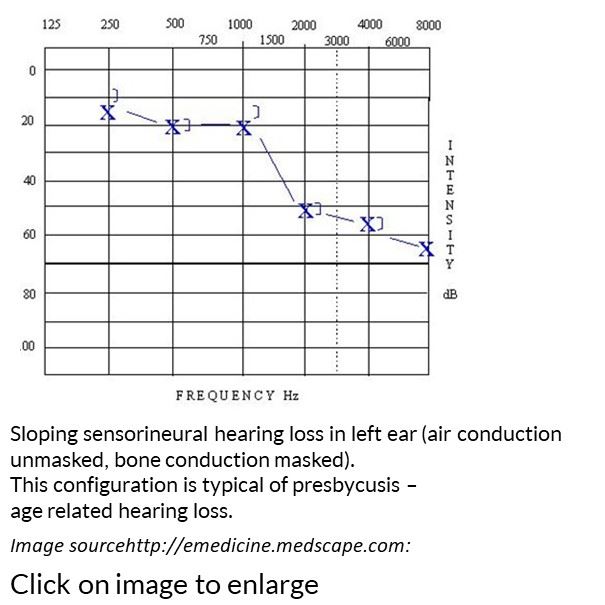
Sensorineural hearing loss will present as a loss of hearing in both air and bone conduction hearing thresholds, whereby air and bone conduction results will be superimposed on each other., within 10 dB. Immittance measures will indicate normal middle ear function, but acoustic reflexes may not be detected if the loss is of moderate degree or worse.
Speech discrimination ability may be reduced relative to those with normal hearing, when tested.
Amplification in the form of hearing devices will be beneficial but if not optimal, cochlear implants may be considered.
Counselling and communication training are necessary adjuncts to using amplification.